 |
Final Report: Governor’s Interagency Coordinating Council on Health Disparities |
Report 17-04, January 2017
Legislative Auditor's Conclusion: The Council meets statutory administrative requirements. Progress on eliminating health disparities is unknown because reports do not track status of recommendations or trends in health disparities.
- Results what we learned
- Report details
- Recommendations and Agency Response
- More about the study
- Contact information
The 2006 Legislature stated its intent “to strive to eliminate health disparities in people of color and between men and women” (2SSB 6197). Health disparities are differences between groups of people in the rate of certain diseases, deaths, or lack of access to health services. The Legislature expressed particular concern about health disparities for women and people of color in comparison to men and the general population.
The Legislature created the Governor’s Interagency Coordinating Council on Health Disparities (Council) within the State Board of Health. The Council is designed to facilitate and report work done by other agencies to address health disparities. The full text of their statutory duties is in RCW 43.20.275 and 43.20.280. The same legislation directed the Joint Legislative Audit and Review Committee (JLARC) to review the Council in 2016.
The Council meets statutory administrative requirements. The Council’s contributions to eliminating health disparities are unclear because the Council’s reports do not clearly and consistently track the status of their recommendations nor discuss trends in specific health disparities.
- The Council meets administrative requirements regarding membership, activities, and timely reporting. For example, it facilitates communication among stakeholders and prioritizes diseases and conditions. The Council is an advisory and planning body that cannot compel agencies to act. Due to confusion over the word “biannual” in the law, the Council has submitted action plan updates twice each year since 2013. The legislative record indicates that the reports are only required once every two years.
- While the Council has submitted reports on time, the reports lack details that would allow the Governor and Legislature to know if the state has made progress on eliminating health disparities. For example, the reports do not provide information about trends in the incidence of the 16 health concerns listed in the original legislation. Further, the reports do not clearly and consistently track whether agencies implemented the Council’s recommendations or the impact of those actions on health disparities.
Recommendations
The Council could better comply with legislative intent by improving the information available about progress on Council recommendations and eliminating health disparities. The Legislative Auditor makes two recommendations regarding the content of Council reports:
- The Council should submit action plan updates every two years with content that reflects the entire prioritized list of health disparities.
- The Council should include the status of all recommendations and all diseases, conditions, and health indicators from the prioritized list in its progress reports.
You can find additional details in the Recommendations tab.
The Governor's Interagency Council on Health Disparities concurs with the Legislative Auditor's Recommendations.
- 1. What is a health disparity?
- 2. Council meets administrative requirements
- 3. Progress on health disparities unknown
- 4. Sunset questions answered
Health Disparity: Groups of people disproportionately affected by certain diseases, rates of death, or access to healthcare
The 2006 Legislature expressed concern regarding health disparities for women and people of color in comparison to men and the general population (2SSB 6197). The Legislature identified 16 diseases and conditions for action by the Governor’s Interagency Coordinating Council on Health Disparities (Council).
The Council complies with administrative requirements set forth in statute
The 2006 Legislature created the Governor’s Interagency Coordinating Council on Health Disparities (Council) within the State Board of Health (Board). The Council is an advisory and planning body, with no direct authority over agencies that implement and regulate health-related programs. The Council has one full-time staff person and receives additional assistance from the Board as needed.
Statute sets administrative requirements for Council membership, activities, and timely reporting. The full text of their statutory duties is in (RCW 43.20.275 and 43.20.280). The Council complies with its administrative requirements, including the following:
- Ensuring diverse membership from state agencies and the public;
- Meeting at least twice per year;
- Facilitating communication and collaboration to address health disparities; and
- Submitting reports on time.
The Council and advisory committees reflect racial, ethnic, and gender diversity
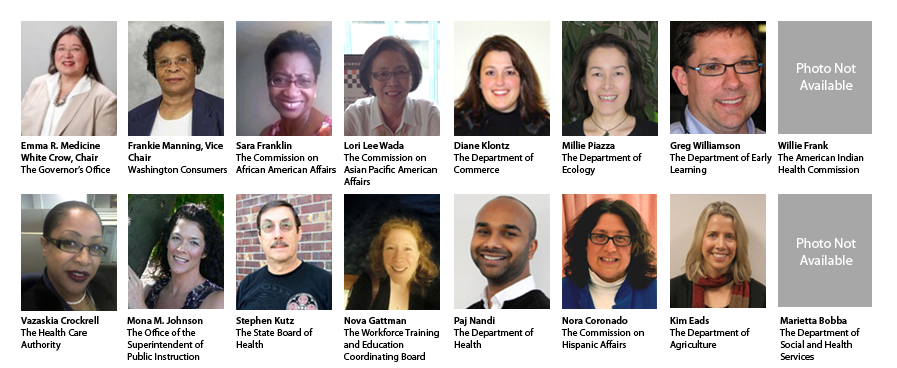
As required by law, the Council has 14 members appointed to represent state agencies, boards, and commissions. It also has 2 members from the public who represent health care consumers, and one member who serves as the Governor’s designee to chair the Council. Membership appears to reflect diversity in race, ethnicity, and gender.
The Council formed advisory committees to address specific conditions. This is required by law. The committees include representatives from state agencies, boards, and commissions and members from the public. The advisory committees reflect diversity in race, ethnicity, and gender.
The Council facilitates communication and collaboration among agencies and stakeholders, and gathers public input
The Council meets about four times each year. At meetings, Council members:
- discuss health disparities and social determinants that affect disparities (e.g., employment, education);
- share ideas about ways to reduce health disparities;
- receive briefings on topics of interest;
- share information about actions their agencies have taken; and
- receive comments from members of the public.
The Council collaborated on a publication that describes ways to produce and distribute health information that is appropriate for various cultures and languages. Council staff and members worked with the Department of Health to create e-learning modules on the Culturally and Linguistically Appropriate Services Standards and provide technical assistance to state agencies to ensure equity is considered in policy and program development. The Council also has collaborated on studies and public forums to better understand how the actions of state government may affect health disparities.
Council submits plans and reports on time. It publishes action plan updates more often than required by law.
Statute required the Council to create an action plan to eliminate health disparities. It also must submit progress reports and updates to the action plan.
- Action plan: The Council produced the action plan in June 2010, more than two years before the December 2012 due date. The action plan is intended to prioritize health disparities and recommend actions that state agencies can take to help eliminate the health disparities.
- Progress reports: As required by statute, the Council submitted progress reports in 2008, 2009, and 2010. These reports discussed the work that led to the action plan. Now that the action plan is complete, progress reports are due every four years in odd-numbered years. These reports should describe the progress made on the recommendations and on eliminating health disparities. The next progress report is due in 2017.
- Action plan updates: JLARC staff inferred from statute that the action plan updates should document changes to the plan. Statute requires the action plan updates be submitted biannually. Biannually can mean twice each year or once every two years. To ensure compliance, the Council has submitted action plan updates twice each year. The Legislative record, however, indicates the Legislature expected the action plan to be updated every two years.
Council does not track recommendations or data about specific health conditions, so progress toward legislative goals is unknown
The 2006 Legislature wanted “to strive to eliminate health disparities in people of color and between men and women.” The Council sets priorities, gathers data, and issues recommendations. The Council does not clearly and consistently report the status of its recommendations or the progress toward eliminating health disparities.
Council is directed to focus on the diseases and conditions specified in statute
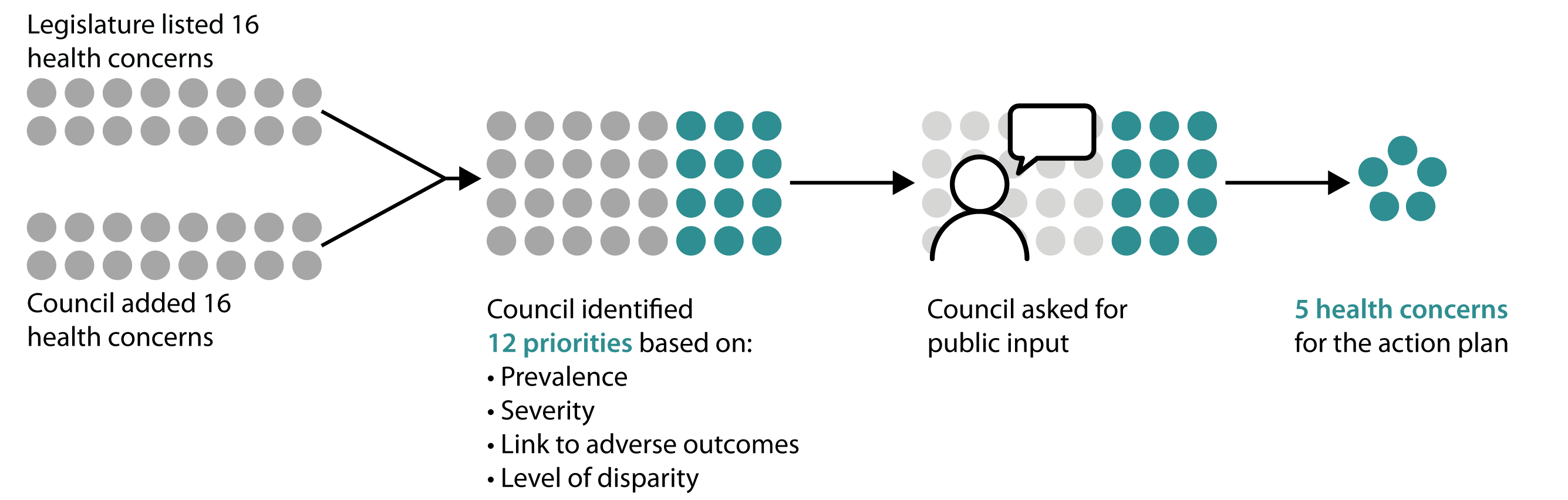
The Council’s action plan must address at least the 16 diseases and conditions listed in statute. Others may be added. The Council must prioritize the list and address it incrementally.
| Diabetes | Asthma | Infant mortality | HIV/AIDS |
| Heart disease | Strokes | Breast cancer | Cervical cancer |
| Prostate cancer | Chronic kidney disease | Sudden infant death syndrome (SIDS) | Mental Health |
| Women's health issues | Smoking cessation | Oral disease | Immunization rates of children and senior citizens. |
For the first action plan in 2010, the Council developed a prioritized list of diseases and conditions. The process involved a Council evaluation and public input. The Council used a similar process in 2012. Starting in 2013, the process used more informal discussions and a priority setting workgroup was convened in 2015.
Council has chosen to focus on social determinants as its approach to addressing the Legislature’s specified health diseases and conditions
The five priorities in the Council’s 2010 action plan were education, health insurance coverage, healthcare workforce diversity, obesity, and diabetes. Of these, only diabetes is named in statute. The action plan also provided recommendations for reducing language barriers and promoting equity within state agencies.
The Council has since chosen to focus on social determinants of health. Social determinants are factors such as level of education and employment that are associated with health disparities. The Council believes that this focus will affect all health disparities including the diseases and conditions listed in statute. In the 2012 action plan update, the Council included a framework linking social determinants with health disparities. The 2012 update also made recommendations regarding behavioral health, environmental exposures and hazards, and poverty.
Later updates included infant mortality, SIDS, and women’s health issues, which are named in statute, as priorities. The Council also began incorporating the Governor’s Health Next Generation initiative priorities into it deliberations in 2015.
Action plan updates do not consistently track data about diseases or conditions
Statute directs the Council to add no more than five diseases and conditions to each action plan update. This approach is designed to keep focus on the Legislature’s concerns and eliminate disparities in the specified areas. However, each update has included a different list of diseases and conditions, so the data is not updated from report to report. Tracking the data over time could better inform how the Council prioritizes its work, and provide feedback on recommendations.
Council’s reports do not clearly and routinely identify and track the status of recommendations made by the Council
The Council includes new recommendations for actions to eliminate health disparities in each plan update. In 2013, the Council provided information about the status of its earlier recommendations. Since then, it has not included information about previous recommendations. As a result, it is unknown whether progress on the recommendations is being made.
Sunset reviews answer four key questions
The law creating the Council required that JLARC staff conduct this review in a manner substantially the same as a Sunset Review (RCW 43.131.071). The statute does not include a termination clause, so unlike a full sunset review, the study did not evaluate if the Council should expire or be renewed.
The Washington Sunset Act (RCW 43.131) directs JLARC staff to answer four specific questions in a sunset review:
1. Has the Council complied with legislative intent?
In part. The Council has been created and is striving to eliminate health disparities, but there are gaps in how the Council is measuring progress toward this goal. To better inform the Legislature, Governor, and public about health disparities, the Council could improve its reporting on the status of Council recommendations and the health disparities.
2. Is the Council operating in an efficient and economical manner?
Yes. The Council is part of the State Board of Health (Board) within the Department of Health serving as the administrative and fiscal agency for the Board. Council expenses in 2016 are estimated at $137,000 predominantly for staff salary and benefits. The Council has one full-time staff person and receives additional assistance from the Board as needed. The Board provides approximately $44,000 in-kind assistance to the Council. Meeting space is typically an in-kind contribution from member agencies. JLARC staff estimate that the agencies, commissions, and boards represented by the Council spend between $15,000 and $20,000 per year for staff time and travel to participate in Council meetings.
Additionally, the Council applied for and received three grants from the U.S. Department of Health and Human Services. These grants provided $1 million between state fiscal years 2008 and 2016. The Council and the DOH, Office of Minority Health used these funds to foster state partnerships to improve minority health.
3. Is the Council reaching expected performance goals and targets?
Yes. The Council created a performance measurement plan for this review that reflects the administrative requirements contained in statute. As noted in Report Details, it has met those administrative requirements.
4. Is the Council duplicating activities by another agency or the private sector?
No. The Council has an overarching function to provide a venue for state agencies and interested parties to come together to share information, coordinate activities, and prioritize efforts to help reduce health disparities. In this respect, there are no other state, public, or private entities engaged in the same coordinating activities or efforts.
The Legislative Auditor makes two recommendations regarding the content of Council reports
The first recommendation addresses action plan updates. It would reduce the frequency of the action plan updates and improve their content. The intended outcome is that Council recommendations and prioritized health disparities would be better communicated and tracked.
The second recommendation addresses progress reports. It would improve the content and organization of the progress reports. The intended outcome is to more clearly and consistently communicate the status of the Council recommendations and health disparities.
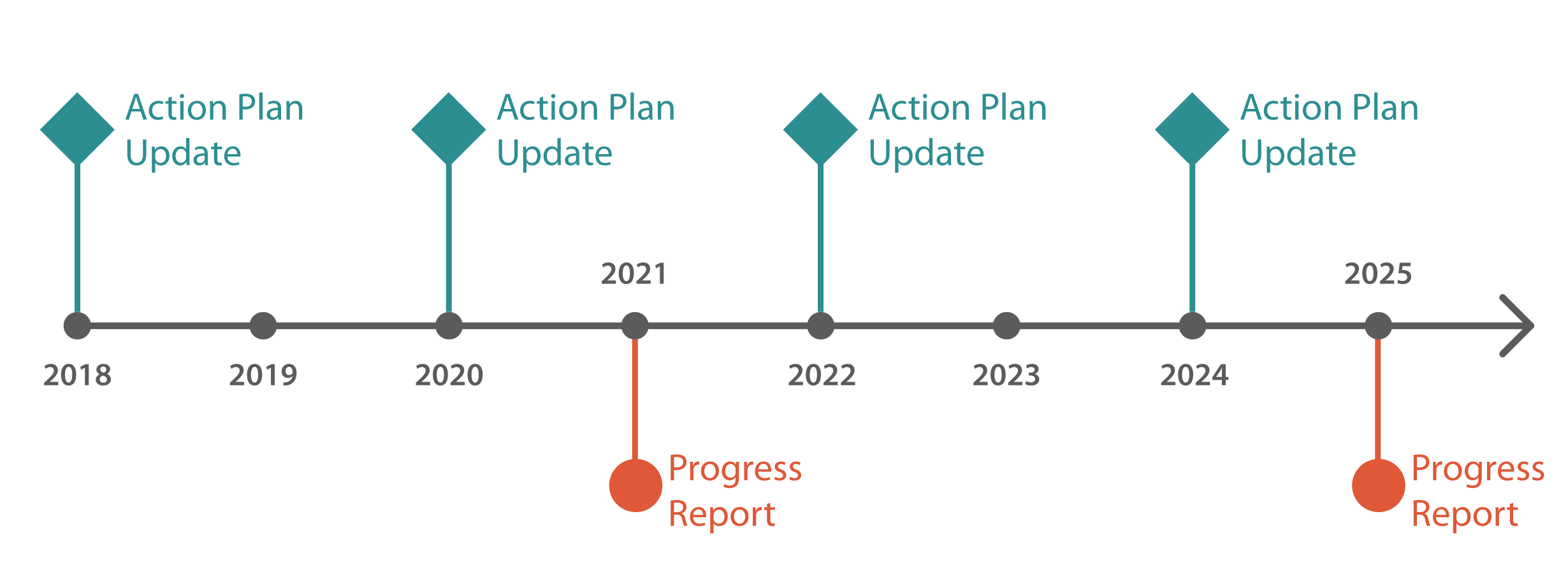
Recommendation #1: The Council should submit action plan updates every two years with content that reflects the entire prioritized list of health disparities.
The Council should revise its current action plan updates, providing them every two years rather than twice per year. The first report would be due in January 2018.
Updates should contain Council recommendations for actions to help eliminate the health disparities on the Council’s prioritized list.
- The prioritized list should include all of the health diseases, conditions, and health indicators found in RCW 43.20.280 and those the Council has elected to add.
- Recommendations should be clearly labeled and numbered.
- Recommendations should include, at a minimum, responsible parties, measures to gauge progress on the recommendations, and timeframes in which the recommendations are to be implemented.
| Legislation Required: | No |
| Fiscal Impact: | None |
| Implementation Date: | January 2018 |
| Agency Response: | Concur - see Agency Response tab |
Recommendation #2: The Council should include the status of all recommendations and all diseases, conditions, and health indicators from the prioritized list in its progress reports.
The Council submits progress reports every four years, in odd numbered years. This should continue.
Beginning in January 2021, progress reports should include the following:
- A section addressing the status of all recommendations made by the Council. It should include progress made on the recommendation since the previous progress report.
- A section addressing the status of the health diseases, conditions, and health indicators found in RCW 43.20.280 as well as those the Council has elected to add. The section should include discussion about the current prevalence rates and any changes in disparities since the previous progress report.
| Legislation Required: | No |
| Fiscal Impact: | None |
| Implementation Date: | January 2021 |
| Agency Response: | Concur - see Agency Response tab |
The Office of Financial Management (OFM) was given an opportunity to comment on this report. OFM responded that it does not have any comments.
Governor's Interagency Council on Health Disparities
Audit Authority
The Joint Legislative Audit and Review Committee (JLARC) works to make state government operations more efficient and effective. The Committee is comprised of an equal number of House members and Senators, Democrats and Republicans.
JLARC's non-partisan staff auditors, under the direction of the Legislative Auditor, conduct performance audits, program evaluations, sunset reviews, and other analyses assigned by the Legislature and the Committee.
The statutory authority for JLARC, established in Chapter 44.28 RCW, requires the Legislative Auditor to ensure that JLARC studies are conducted in accordance with Generally Accepted Government Auditing Standards, as applicable to the scope of the audit. This study was conducted in accordance with those applicable standards. Those standards require auditors to plan and perform audits to obtain sufficient, appropriate evidence to provide a reasonable basis for findings and conclusions based on the audit objectives. The evidence obtained for this JLARC report provides a reasonable basis for the enclosed findings and conclusions, and any exceptions to the application of audit standards have been explicitly disclosed in the body of this report.
Committee Action to Distribute Report
On January 4, 2017 this report was approved for distribution by the Joint Legislative Audit and Review Committee.
Action to distribute this report does not imply the Committee agrees or disagrees with Legislative Auditor recommendations.
Scope & Objectives
Why a JLARC Review of the Governor’s Interagency Council on Health Disparities?
In 2005, the Legislature’s Joint Select Committee on Health Disparities issued a report that identified health disparities for certain conditions and diseases, highlighted social determinants, and called for the creation of an interagency coordinating council.
In 2006, the Legislature created the Governor’s Interagency Council on Health Disparities (SSB 6197). The legislation identified the work to be done by the Council and directed the Joint Legislative Audit and Review Committee (JLARC) to review the Council and its functions.
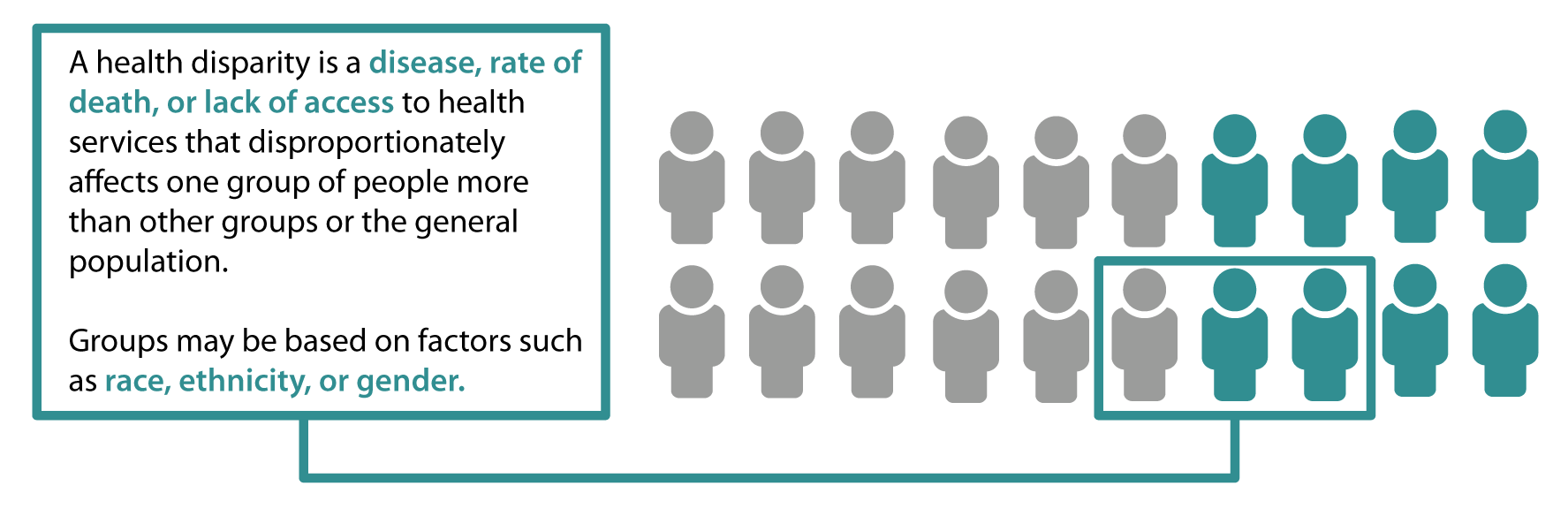
What are Health Disparities?
Health disparities refer to differences between population groups in the rate of certain diseases, rate of deaths from those diseases, or lack of access to health services. These groups may be based on factors such as race, ethnicity, or gender. Studies have shown that social determinants such as education and employment are associated with health disparities.
In stating its intent, the Legislature expressed particular concern regarding health disparities for women and people of color in comparison to men and the general population.
Council Membership and Responsibilities
The 17-member Council is housed at the State Board of Health, which provides staff and funding. Council members represent state agencies and commissions, as well as the public. The Council must reflect diversity in race, ethnicity, and gender.
The Legislature directed the Council to perform the following work:
- Promote and facilitate communication, coordination, and collaboration among relevant state agencies and other private or public stakeholders to address health disparities;
- Gather information to understand how the actions of state government improve or contribute to health disparities;
- Assess and recommend initiatives for improving availability of culturally appropriate health literature and interpretive services at public and private health-related agencies;
- Create and regularly update an action plan and statewide policy to address factors that lead to health disparities;
- Establish advisory committees that reflect diversity in race, ethnicity, and gender; and
- Provide regular progress reports to the Governor and Legislature.
Study Scope
JLARC staff will review and report on the operations and progress of the Governor’s Interagency Council on Health Disparities. As directed in law, the review will use a process substantially the same as a sunset review (RCW 43.131.071). However, since the statute does not include a termination clause, the JLARC staff report will not evaluate if the Council should be terminated.
Study Objectives
JLARC staff will address the following objectives:
- To what extent has the Council complied with legislative intent, including requirements for diverse membership, culturally appropriate health literature, timely reporting, and action plan development?
- To what extent does the Council provide for efficient and economical operations?
- To what extent have the Council’s actions achieved expected performance goals and targets?
- To what extent does the Council duplicate the activities of another agency or the private sector?
Timeframe for the Study
Staff will present the preliminary report at the JLARC meeting in December 2016. The final report will be presented at the JLARC meeting in January 2017.
Study methodology
The methodology JLARC staff use when conducting analyses is tailored to the scope of each study, but generally includes the following:
- Interviews with stakeholders, agency representatives, and other relevant organizations or individuals.
- Site visits to entities that are under review.
- Document reviews, including applicable laws and regulations, agency policies and procedures pertaining to study objectives, and published reports, audits or studies on relevant topics.
- Data analysis, which may include data collected by agencies and/or data compiled by JLARC staff. Data collection sometimes involves surveys or focus groups.
- Consultation with experts when warranted. JLARC staff consult with technical experts when necessary to plan our work, to obtain specialized analysis from experts in the field, and to verify results.
The methods used in this study were conducted in accordance with Generally Accepted Government Auditing Standards.
More details about specific methods related to individual study objectives are described in the body of the report under the report details tab or in technical appendices.
Contact
Authors of this Study
John Bowden, Research Analyst, 360-786-5298
Eric Whitaker, Research Analyst, 360-786-5618
Valerie Whitener, Audit Coordinator
Keenan Konopaski, Legislative Auditor
Joint Legislative Audit and Review Committee
Eastside Plaza Building #4, 2nd Floor
1300 Quince Street SE
PO Box 40910
Olympia, WA 98504-0910
Phone: 360-786-5171
FAX: 360-786-5180
Email: JLARC@leg.wa.gov
JLARC Members on Publication Date
Senators
Randi Becker
John Braun, Chair
Sharon Brown
Annette Cleveland
David Frockt
Bob Hasegawa
Mark Mullet, Assistant Secretary
Representatives
Jake Fey
Larry Haler
Christine Kilduff
Drew MacEwen
Ed Orcutt, Secretary
Gerry Pollet
Derek Stanford, Vice Chair
Drew Stokesbary